| University of Bielefeld - Faculty of technology | |
|---|---|
|
Networks and distributed Systems
Research group of Prof. Peter B. Ladkin, Ph.D. |
|
| Back to Abstracts of References and Incidents | Back to Root |

 PB86-910403
PB86-910403
WASHINGTON, D.C. 20594
| 1. Report No.: NTSB/AAR-86/03 | 2. Government Accession No.: PB86-910403 | 3. Recipient's Catalog No.: | |
| 4. Title and Subtitle: Aircraft Accident Report-- China Airlines Boeing 747-SP, N4522V, 300 Nautical Miles Northwest of San Francisco, California, February 19. 1985 | 5. Report Date: March 29, 1986 | ||
| 6. Performing Organization: Code | |||
| 7. Author(s): | 8. Performing Organization : Report No.: | ||
| 9. Performing Organization Name and Address : National Transportation Safety Board Bureau of Accident Investigation Washington, D.C. 20597 | 10. Work Unit No.: 433A | ||
| 11. Contract or Grant No.: | |||
| 13. Type of Report and Period Covered: Aviation Accident Report February 19, 1985 | |||
| 12. Sponsoring Agency Name and Address : NATIONAL TRANSPORTATION SAFETY BOARD Washington, D.C. 20594 | |||
| 14. Sponsoring Agency Code : | |||
| 15. Supplementary Notes : | |||
| 16. Abstract : About 1016 Pacific standard time, February 19, 1985, China Airlines Flight 006, a Boeing 747 SP-09, enroute to Los Angeles, California from Taipei, Taiwan, suffered an inflight upset. The flight from Taipei to about 300 nmi northwest of San Francisco was uneventful and the airplane was flying at about 41,000 feet mean sea level when the No. 4 engine lost power. During the attempt to recover and restore normal power on the No.4 engine, the airplane rolled to the right, nosed over, and entered an uncontrollable descent. The captain was unable to restore the airplane to stable flight until it had descended to 9,500 feet. After the captain stabilized the airplane, he elected to divert to San Francisco International Airport, where a safe landing was made. Although the airplane suffered major structural damage during the upset, descent, and subsequent recovery, only 2 persons among the 274 passengers and crew on board were injured seriously. The National Transportation Safety Board determines that the probable cause of this accident was the captain's preoccupation with an inflight malfunction and his failure to monitor properly the airplane's flight instruments which resulted in his losing control of the airplane. Contributing to the accident was the captain's over-reliance on the autopilot after the loss of thrust on the No. 4 engine. | |||
| 17. Key Words: Loss of engine thrust, inflight upset distraction, instrument scan, failure to monitor instruments, over reliance on the autopilot | 18. Distribution Statement This document is available to the public through the National Technical Information Service, Springfield, Virginia 22161 | ||
| 19. Security Classification (of this report) UNCLASSIFIED | 20. Security classification : (of this page) UNCLASSIFIED | 21. No. of Pages : 48 | 22. Price : |
| SYNOPSIS | 1 | |
| 1. | FACTUAL INFORMATION | 1 |
| 1.1 | History of the Flight | 1 |
| 1.2 | Injuries to Persons | 5 |
| 1.3 | Damage to Aircraft | 6 |
| 1.4 | Other Damage | 6 |
| 1.5 | Personnel Information | 6 |
| 1.6 | Airplane Information | 6 |
| 1.7 | Meteorologica1 Information | 7 |
| 1.8 | Aids to Navigation | 7 |
| 1.9 | Communications | 8 |
| 1.10 | Aerodrome Information | 8 |
| 1.11 | Flight Recorders | 8 |
| 1.11.1 | Digital Flight Data Recorder Information | 9 |
| 1.12 | Wreckage and Impact Information | 12 |
| 1.13 | Medical and Pathological Information | 13 |
| 1.14 | Fire | 14 |
| 1.15 | Survival Aspects | 14 |
| 1.16 | Tests and Research | 15 |
| 1.16.1 | Powerplants | 15 |
| 1.16.2 | Human Performance Information | 16 |
| 1.17 | Other Information | 20 |
| 1.17.1 | Airplane A.C. Electrical System | 20 |
| 1.17.2 | Automatic Flight Systems | 21 |
| 1.17.3 | JT9D-7A Engine Operating Procedures | 22 |
| 1.17.4 | Engine-out Training and Flight Procedures | 23 |
| 1.17.5 | Actions Taken by the Additional Flightcrew Members | 24 |
| 2. | ANALYSIS | 25 |
| 2.1 | The Engine Failure | 25 |
| 2.2 | The Flightcrew | 28 |
| 3. | CONCLUSIONS | 33 |
| 3.1 | Findings | 33 |
| 3.2 | Probable Cause | 34 |
| 4. | RECOMMENDATIONS | 34 |
| 5. | APPENDIXES | 35 |
| 5.1 | Appendix A--Investigation and Hearing | 35 |
| Appendix B--Personnel Information | 36 | |
| Appendix C--Airplane Information | 38 | |
| Appendix D--Applicable Boeing 747 SP Engine Malfunction Checklists | 39 |
About 1016 Pacific standard time, February 19, 1985, China Airlines Flight 006, a Boeing 747 SP-09, enroute to Los Angeles, California from Taipei, Taiwan, suffered an inflight upset. The flight from Taipei to about 300 nmi northwest of San Francisco was uneventful and the airplane was flying at about 41,000 feet mean sea level when the No. 4 engine lost power. During the attempt to recover and restore normal power on the No. 4 engine, the airplane rolled to the right, nosed over, and entered an uncontrollable descent. The captain was unable to restore the airplane to stable flight until it had descended to 9,500 feet. After the captain stabilized the airplane, he elected to divert to San Francisco International Airport, where a safe landing was made. Although the airplane suffered major structural damage during the upset, descent, and subsequent recovery, only two persons among the 274 passengers and crew on board were injured seriously.
The National Transportation Safety Board determines that the probable cause of this accident was the captain's preoccupation with an inflight malfunction and his failure to monitor properly the airplane's flight instruments which resulted in his losing control of the airplane.
Contributing to the accident was the captain's over-reliance on the autopilot after the loss of thrust on the No.4 engine.
1.1 History of the Flight
China Airlines Boeing 747 SP-09, Flight 006, was a regularly scheduled passenger flight between Taipei, Taiwan, and Los Angeles, California. Flight 006 departed Taipei at 0022 Pacific standard time 1/ (1622 Taipei local time), February 19, 1985, with 251 passengers and 23 crewmembers on board.
The flight was uneventful until just west of reporting point Redoo, about 300 nmi northwest of San Francisco, California. Flight 006 was at flight level (FL) 410 2/ and was estimating Redoo at 1013. The flight was above a lower cloud layer
whose tops were reported to be at or about 37,000 feet. 3/ The airplane's autopilot was engaged and was operating in the Performance Management System (PMS) mode. The PMS was providing pitch guidance and maintaining a selected 41,000 feet; roll guidance to the autopilot was provided by the Inertial Navigation System (INS). The autopilot uses only the airplane's ailerons and spoilers for lateral control; it does not use the airplane's rudder and rudder trim for this purpose. The PMS also was maintaining 0.85 Mach (M), 254 knots indicated airspeed (KIAS), by providing thrust setting commands to the airplane's autothrottle system servomotor. According to the flightcrew, as the airplane approached Redoo, it began to encounter light clear air turbulence. The airspeed began fluctuating between about 0.84 (251 KIAS) and 0.88M (264 KIAS) and the PMS began moving the throttles forward and aft to maintain the commanded cruise Mach number (0.85 M).
About 1010, the Mach number increased to about 0.88 M, the PMS retarded the throttles, engine thrust decreased to about 1.0 EPR 4/, and the airplane began decelerating. As the airspeed reached about 0.84M, the PMS moved the throttles forward. Engines 1, 2, and 3 responded to the movement of the throttles and began accelerating; however, the flight engineer said that the instrument gauges of the No. 4 engine did not indicate a corresponding acceleration. The flight engineer then moved the No. 4 throttle forward and aft manually, but he said that he did not see any corresponding indication of engine response to the throttle movements on the applicable engine instruments. At the time this occurred, the flight engineer said that the four main tanks were supplying fuel directly to their respective engines. The No. 2 main tank was pressurizing the fuel crossfeed system; all other fuel tank crossfeed valves were closed. The automatic fuel heating system was on. In addition, the captain had turned the "fasten seatbelt" signs on when the flight had encountered the clear air turbulence. In accordance with company procedures, the flight engineer had placed the ignition switches in the "flight start" position, thereby providing continuous ignition to all four engines. At the time of the occurrence, and in accordance with the company's procedures, two of the airplane's three air conditioning packs were on and set to the "half flow" position.
The captain said that he observed the flight engineer move the No. 4 throttle. He said that he did not "feel" anything unusual when the No. 4 engine did not accelerate; he just noticed that the No. 4 engine's instrument gauges were not responding to the throttle movements and that the indicated airspeed began decreasing.
Shortly thereafter, the flight engineer told the captain that the No. 4 engine had flamed out. The flight engineer said that he also noted that the No. 4 generator breaker open light on the electrical section of the flight engineer's instrument panel was lit, indicating that the No. 4 generator control breaker had opened and the generator was no longer on-line. Thereafter, in response to the captain's command, he took out his checklist to review the applicable engine out procedures and the airplane performance charts to ascertain the three-engine enroute cruise altitude. The captain directed the first officer to request a lower altitude from air traffic control (ATC) in order to descend and to restart the engine. Although the maximum engine restart altitude is 30,000 feet, the captain directed the flight engineer to try to relight the No. 4 engine while at 41,000 feet. The flight engineer placed the engine's No. 2 ignition switch to the "flight start" position, thus putting both ignition systems on the No. 4 engine in continuous ignition. (Only one of the two ignition systems are used during normal operations.
According to company procedures, the No. 1 system is used eastbound and No. 2 westbound.) The attempt was unsuccessful and the airplane continued to decelerate.
The first officer heard the flight engineer tell the captain that the No. 4 engine had flamed out and he told the relief flight engineer to come forward and help the "on duty" flight engineer. He saw that the airspeed was decreasing and he informed the captain of the situation. At 1014:11, he requested a lower altitude from the Oakland, California, Air Route Traffic Control Center (ARTCC). He did not tell Oakland ARTCC about the engine failure, nor did he declare an emergency. The first officer said that Oakland ARTCC told him to "stand by" and he did not recall hearing anything further in response to his request. However, the ATC transcript showed that, at 1015:01, Oakland ARTCC had cleared the flight to descend to and to maintain FL 240 and that Flight 006 did not acknowledge the clearance. In addition, between 1015:13 and 1016:28, Oakland ARTCC tried unsuccessfully six times to contact Flight 006.
The captain said that the airspeed dropped through 240 KIAS, and, as the airplane continued to decelerate, he turned the autopilot's speed mode selector switch from PMS to "OFF" to release it from the altitude hold command. This switched the autopilot to the pitch attitude hold mode while maintaining the INS track in the autopilot roll mode without any pilot input. He then rotated the pitch control wheel on the autopilot manual control module in the nose-down direction to begin a descent to arrest the airspeed loss; however, the captain said that the airspeed continued to decrease and so he disengaged the autopilot to lower the airplane's nose manually at a faster rate in a further attempt to arrest the airspeed loss.
The first officer stated that he "looked up" after he completed his radio call and saw that the airplane had banked "slightly" to the right. He said that he saw the captain disconnect the autopilot, that the airplane continued to bank to the right, and that he "told the captain it was banking right."
The captain said that after he disengaged the autopilot the airplane yawed and rolled further right and that the first officer told him that the airplane "was banking right." He said that while he was concentrating on his attitude director indicator (ADI) to make a left-wing-down correction, the instrument's background, which contained the horizon reference line, rotated rapidly to the left and the horizon reference line rolled to the vertical position. The captain said that he did not see any failure flags or lights on his ADI and when he looked over at the first officer's ADI and the standby ADI 5/, they looked the same as his. By this time, according to the captain, the airplane had entered the clouds, and he didn't know what attitude it was in.
The captain said that about the time the ADIs rotated, the flight engineer told him that the other three engines had lost thrust and that the "airplane dropped all of a sudden." He pulled back on the control column, but the indicated airspeed continued increasing rapidly until it exceeded the airplane's maximum operating speed (Vmo) 6/. During this part of the "upset," the first officer said that his ADI had rotated to the left in the same manner as the captain's and that he did not see any ADI failure flags or lights. He said that, at that point in the flight, he saw that both the captain's and his ADIs "had malfunctioned," that the airplane was out of control, banking left and right, and that he felt that it was in a steep bank.
The flight engineer said that he felt the airplane enter an abnormal attitude, he heard the captain report that his ADI was lost, and he saw the standby ADI "going out of limits." He said that the airplane was descending and the captain was trying to recover when he saw the No. 1, 2, and 3 engines had lost thrust. After telling the captain, he moved the three throttles forward and aft, but he did not observe any corresponding indications of thrust response on the engine's instruments. He placed the standby ignition switch "on" but there was no engine response. Thereafter, the G forces became so great that he could not lift his arms and his head was forced down against the center control pedestal. (The standby ignition switch uses the standby bus alternating current (a.c.) electrical power. The standby a.c. bus is normally supplied by the essential a.c. bus. As an alternate, the power can be supplied from the battery/static inverter. Placing the selector switch to either the "IGN 1" or the "IGN 2" position provides continuous ignition to all engines through the selected igniter when the start levers are in the rich or idle position.)
The captain stated that he was unable to recover the airplane while it was in the clouds; he was uncertain of its roll attitude and was moving the control wheel to the left and to the right. However, as the airplane accelerated, the captain said he continued to pull the control column back and the airplane began to decelerate rapidly. The captain said that the airspeed decreased to between about 80 to 100 KIAS and, at that point, he lowered the airplane's nose, the airplane accelerated, and the indicated airspeed again exceeded Vmo. The captain, then assisted by the first officer, pulled the control column back and the airplane decelerated. The captain lowered the nose smoothly. The airplane began accelerating slowly and as it did so, it emerged from the clouds. The captain told the flightcrew that he could see the horizon outside the airplane. The captain, first officer, and flight engineer said that they did not hear the overspeed aural warning and that the stall warning stickshaker did not activate at any time during the descent.
As the airplane emerged from the clouds at about 11,000 feet it was, according to the captain, accelerating through 180 KIAS. The captain, based on outside visual references, began regaining control and was able to finally stabilize the airplane at about 9,500 feet. The first officer said that he saw his ADI was "coming back" just before the captain announced that he could see the horizon outside the airplane. The flight engineer also noted that he saw the first officer's ADI "coming in" at this time.
As the airplane descended through 10,000 feet, the flight engineer said that the Nos. 1, 2, and 3 engines "came in," but the No. 4 engine did not start. When he placed the No. 4 ignition switch in the ground start position, however, the engine did start. According to the flight engineer, the restart of the No. 4 engine was accomplished in accordance with checklist procedures.
The flight engineer stated that he did not think that the airplane lost a.c. electrical power during the upset and subsequent descent. He said that he had not seen any instrument warning flags during the entire episode and that, "If we had lost electrical power we would have seen flags." According to the flight engineer, after all the engines had started, he checked the electrical control panel, and, except for the fact that the No. 4 generator open light was lit, all other lights were out and "everything was normal." He closed the No. 4 generator control breaker, the light went out, and the generator came on line.
After the airplane was stabilized, Oakland ARTCC was contacted, and, at 1017:03, Flight 006 reported that it had experienced a "flameout, ah, we emergency... .we are niner thousand feet.. ." Thereafter, the flight requested and was
given radar vectors to return to course. At 1018:42, Flight 006 requested clearance to climb. Oakland ARTCC initially cleared it to climb to FL 200, and, at 1019:17, Flight 006 told the ARTCC that "we can control the aircraft." Oakland ARTCC asked the flight if it wanted to divert to San Francisco, and, at 1019:49, Flight 006 answered "Condition normal now," and that it would continue to Los Angeles. Flight 006 was then cleared to climb to and maintain FL 350. While the airplane was climbing, the flight engineer checked his instrument panel. The body gear door open annunciator lights and the body landing gear down lights were on, indicating that the doors were open and the body landing gear were down and locked. In addition, the No. 1 hydraulic system fluid level gauge indicated empty.
Because of the landing gear indications, the captain elected to level off at FL 270 with the gear extended. (The maximum operating altitude for flight with the landing gear extended is 29,000 feet.) After checking the airplane's fuel status and fuel consumption at 27,000 feet with the gear extended, the captain decided to divert to San Francisco and instructed the first officer to inform Oakland ARTCC of their intentions. At 1035:34, Oakland ARTCC cleared Flight 006 to San Francisco via Point Reyes, California, and to maintain FL 270.
At 1038:39, Flight 006 redeclared an emergency and stated that there were injured people onboard. At 1038:54, Oakland ARTCC cleared the flight direct to San Francisco and to descend at "pilot's discretion." The descent into San Francisco was made with the autopilot engaged and it operated satisfactorily until it was disengaged at 2,500 feet while on a long final approach to runway 28L at San Francisco International Airport. The remaining landing gear and the flaps were lowered manually in accordance with prescribed checklist procedures. In addition, the engines all operated normally throughout the climb to FL 270, the cruise at FL 270, the descent, and landing.
After landing, the captain cleared the active runway. Because of the inoperative No. 1 hydraulic system which decreased his ability to steer the airplane during taxi, the captain stopped the airplane after it was clear of the active runway, the engines were shut down, and the airplane was towed to the gate.
1.2 Injuries to Persons
| Injuries | Crew | Passengers | Others |
| Fatal | 0 | 0 | 0 |
| Serious | 1* | 1* | 0 |
| Minor/None | 22 | 250 | 0 |
| Total | 23 | 251 | 0 |
*One cabin crew member received an acute back strain. On February 19, 1985, he was admitted to a hospital and was hospitalized for more than 48 hours. The passenger suffered lacerations and bone fractures on his right foot. Both injuries were classified as serious in accordance with Section 49 CFR 830.2 of the Safety Board's rules. Section 830.2 defines serious injuries, in part, as follows:
1.3 Damage to the Airplane
The airplane was damaged substantially (see section 1.12).
1.4 Other Damage
No other property damage resulted from this accident.
1.5 Personnel Information
A five-man flightcrew was on board for this flight. In addition to the primary three-man flightcrew, a relief captain and flight engineer were assigned to the flight. All flightcrew members were qualified and trained in accordance with applicable Chinese and United States regulations and prescribed China Airlines' procedures. The examination of the flightcrew's training records did not disclose anything out of the ordinary. (See appendix B.)
The primary flightcrew's captain and first officer had served in their country's air force before joining China Airlines. Neither pilot flew fighter type aircraft while in the air force and neither had done any aerobatic work since completing their air force training.
1.6 Airplane Information
The aircraft for Flight 006, a Boeing 747 SP-09, N4522V, was owned by the Wilmington Trust Company, Wilmington, Delaware, and was leased and operated by China Airlines. The airplane was powered by four Pratt & Whitney JT9D-7A engines. The airplane was maintained in accordance with applicable Chinese Civil Aviation Administration and United States Federal Aviation Administration (FAA) regulations, and also with China Airlines maintenance procedures. (See appendix C.) The airplane's weight and center of gravity locations were within applicable weight and balance limitations throughout the entire flight. At the time of the occurrence, the airplane weighed about 440,000 pounds. At this weight, the airplane's three-engine long range cruise altitude was 37,000 feet and its stall speed was about 155 KIAS.
The inspection of the airplane's flight logbook showed that the No. 4 engine had been written up on two previous flights. On February 15, 1985, the logbook indicated that the No. 4 engine lost thrust "when reducing thrust to idle at (FL) 410. Restart, resume to normal (sic) at FL 300." The logbook's corrective action taken column contained the following: the engine was inspected visually, the fuel filter was drained, and the engine vane controller was inspected and "checked Ok."
On February 18, 1985, the No. 4 engine again lost thrust, this time "when reducing thrust to idle at (FL) 430. Engine power failed to response (sic) moving thrust lever. Check F/F (fuel flow) low. Restart at (FL) 280. Resume (normal operation)." The logbook's corrective action taken column contained the following: the water drains from the mach probes manifold, the engine vane controller, the pressure hydraulic fuel filter elements, and air fuel converter were replaced; the fuel pump water filter drain was checked and found to be "normal"; and the results of a subsequent engine run up were "normal."
In addition, during the preflight inspection before the accident flight, the following malfunction was found and entered in the logbook: "No. 4 engine high stage (bleed air) valve light illuminated." The corrective action entry showed that the bleed valve was removed and replaced before the flight.
1.7 Meteorologica1 Information
The National Weather Service's (NWS) 1000 surface weather map showed an area of low pressure over northern British Columbia and Alberta, Canada, and a large high over the northern Pacific Ocean area centered at 40� north latitude, 140� west longitude. A trough extended out of the low along the northwest Pacific coast with a cold front extending south along the coast from near Vancouver, Canada to southern Oregon and then turning west into the Pacific Ocean.
The 0400 200 millibar map (about 38,700 feet) showed a shallow trough in the westerlies extending south-southwest out of northern British Columbia into the Pacific Ocean. The centerline of the trough was about 500 nmi west of the northern California coast. A jet stream core containing wind velocities exceeding 90 knots was located on the upwind side of the trough. The wind flow in the vicinity of the accident was westerly at about 40 knots.
The 1600 200 millibar map showed that the trough had deepened and its centerline had moved just east of the northwest U.S. Pacific coast. The jet stream core was still on the upwind side of the trough with the perimeter of the 70 knot winds in the vicinity of the accident. The maximum observed wind was 160 knots about 900 nmi northwest of the accident site. Based on this pattern, the winds in the vicinity of the accident site would have been from the northwest at 70 knots.
The 1431 Geostationary Operational Environment Satellite (GOES) infrared photograph showed the location of the accident to be on the eastern edge of a cloud area which closely paralleled the surface cold front. Based on the infrared shading curve, the visible clouds appeared to be cirrus (high ice crystal clouds).
The 1100 National Weather Service sounding at Medford, Oregon showed a double tropopause with temperature minima of -67.5�C at 38,050 feet and -67.�C at 56,525 feet. The temperature at a flight altitude of 41,000 feet was -64.6�C.
Between 0752 and 1138, 11 pilot reports were received from flights transitting the area of the accident at altitudes between FL 370 and FL 410. They reported temperatures between -61�C and -64�C, and northwesterly winds ranging from 45 knots to 114 knots.
The examination of the dispatch package showed that the weather information provided to the flightcrew of Flight 006 included the forecast winds aloft enroute, a high level significant weather prognostic map, 200 and 300 millibar prognostic maps, and the TAFORs (International Terminal Forecasts) for Los Angeles, San Francisco, and Oakland.
1.8 Aids to Navigation
Not applicable.
1.9 Communications
There were no known communications malfunctions.
1.10 Aerodrome Information
San Francisco International Airport, elevation 10 feet, is located 8 miles southeast of downtown San Francisco, and is served by eight runways. Runway 28L is 10,600 feet long and 200 feet wide, and has an asphalt surface.
1.11 Flight Recorders
The airplane was equipped with a Fairchild A-100 cockpit voice recorder (CVR), Serial No. 15119. The CVR was brought to the National Transportation Safety Board's Washington, D.C. Audio Laboratory for readout. The recorder contained an excellent quality 30-minute recording; however, the recorder was allowed to run throughout the entire flight and the elapsed time between the accident and landing exceeded the recording medium's 30-minute capability. In addition, the CVR was allowed to continue recording after the airplane had landed. Since the recording tape contained no pertinent information, no transcript was prepared.
The airplane was equipped with a Lockheed Air Services Model 209E Digital Flight Data Recorder (DFDR), Serial No. 717. The recorder was removed and sent to the Safety Board's Washington, D.C. laboratory for readout. The DFDR was undamaged and in working order on arrival.
The DFDR data contained VHF radio microphone keying data. These data were correlated to the times contained on the ATC transcript of communications between Flight 006 and Oakland ARTOC to establish a real time reference for the various events contained on the DFDR readout. The timing correlation is accurate to within 1 second.
Computer Animation.--A real-time animation of a line drawing of an airplane, driven by selected flight recorder parameters, was prepared. The animation covers 6.5 minutes of the flight from 1008:53 to 1015:23, when DFDR data was lost (see section 1.11.1). The animation displays an airplane model flying over the surface of the earth (a 10-nautical mile grid), plus altitude, airspeed, heading, control wheel position, and time in digital format. It also contains an analog display of control wheel position and EPR. The parameters of pitch, roll, and derived ground track are shown via the computer generated model. The ground track was developed using the forecast winds, temperatures, and the DFDR recorded altitude, airspeed, and heading values. ATC communications on the audio are synchronized with the video display.
The airplane model is positioned in the center of the screen while the grid depicting the surface of the earth moves to show groundspeed, track, and attitude. The viewer is positioned 300 feet behind and 50 feet above the center of the model with a viewing angle equal to the magnetic heading. The DFDR data were interpolated linearly in 1/14-second intervals to produce a smooth real-time presentation. The 1/14-second interval was dictated by the limitations of the Safety Board's computer hardware.
The presentation depicts the loss of thrust from the No. 4 engine at 40,900 feet. It also shows the increasing left-wing-down control wheel offset to counteract the increasing asymmetric force resulting from the loss of thrust, until the maximum control wheel offset available to the autopilot is reached. The presentation
shows that the airplane pitched down and rolled to the right. The nosedown pitch angle reached 69� and, by the time the airplane had descended to 30,000 feet, it had almost completed a 360� right roll and had pitched upward to about 11� nosedown pitch attitude. (Figures 1-7 were extracted from the computer animation.)
1.11.1 Digital Flight Data Recorder Information
Recorder Data Losses.--The examination of the DFDR readout disclosed a number of periods where data were lost. These data losses were the result of the vibration and the sustained vertical acceleration forces (Gs) exerted on the recorder during the descent. Some of these data were retrieved through the use of recovery techniques, but the accuracy of these recovered data is suspect. In addition, anomalies in the recorded altitude and airspeed values appeared early in the descent because the descent rate of the airplane had exceeded the maximum tracking capability of the airplane's digital air data computer (DADC). Specific details are discussed below.
The first sustained data loss occurred at 1015:23 as the airplane was descending through 30,132 feet at 296 KIAS 7/ and the vertical acceleration values approached 5 Gs. Thereafter, invalid data was recorded for several periods during the early part of the descent.
Between 1016:08 and 1016:14, and between 1016:23 and 1017:12 during the descent, the synchro parameters for altitude (two synchros), indicated airspeed, heading, pitch, and roll displayed erroneous data, whereas the synchro parameters for the flaps, stabilizer position, control wheel position, and angle of attack were recorded correctly. The ten synchro inputs discussed above are divided into two groups: Group 1 contained the six synchros that displayed erroneous data; Group 2 contained the four synchros that displayed correct data. Power for the Group 1 synchros is routed through the standby ignition switch from the standby a.c. bus, which is normally powered by the essential AC bus. Placing the standby ignition switch at either standby ignition number 1 or number 2 will cut off power to the Group 1 synchros. The Group 2 synchros receive their power directly from the essential a.c. bus. As noted earlier, the flight engineer had placed the standby ignition switch to either the number 1 or the number 2 ignition system during the descent.
DFDR Readout Information.--At 1010:06, the DFDR data showed that the airplane was at 41,006 feet, that all four engine EPRs were about 1.4, and that the airplane was accelerating through 258 KIAS. About 1010:08, the engine pressure ratios began decreasing, but the airplane continued to accelerate until, at 1010:36, it was indicating 264 KIAS. As the EPRs continued to decrease, the airplane began to decelerate. By 1010:46, the EPRS had decreased to about 0.9, and at 1011:05, the airplane had slowed to about 255 KIAS. The wings were essentially level and the control wheel was centered. At these altitudes and at 0.84M, the EPR at idle rpm should be about 0.7 to 0.75; the windmilling EPR should be about 0.05 to 0.07 lower than the idle EPR.
At 1011:10, after the airspeed had decreased to about 251 KIAS, the EPRs on engines 1, 2, and 3 began increasing and, by about 1011:30, they had reached about 1.5 EPR. (At 41,000 feet, 0.85M, and with two air conditioning packs operating, the "max cruise" EPR limit is 1.543 EPR.) Thereafter, these three EPRs remained at about 1.5 until shortly after the start of the upset. During this period, the No. 4 engine's EPR
increased from 0.9 to about 1.02 and remained fairly constant at that reading until 1012:06. Between 1012:06 and 1012:41, the No. 4 EPR increased slightly to about 1.05.
Between 1011:10 and 1012:38, the airspeed fluctuated between 248 KIAS and 253 KIAS and then stabilized at about 250 KIAS. The airplane's roll angle increased from 0.3� to about 2� left-wing-down and the control wheel began deflecting left until, at 1012:30 it stabilized at about a 7� left-wing-down deflection.
At 1012:40, the No. 4 engine's EPR began decreasing and from 1012:45 to 1013:05, the DFDR recorded EPR readings ranging from 0.83 to 0.69, but by 1013:10, the reading had increased to about 1.01 EPR. During this 30-second period, the other three engines were stabilized at essentially 1.5 EPR; the airspeed decreased from 251 KIAS to 243 KIAS, and, although the airplane remained at 40,900 feet in a 3� left-wing-down attitude, the left-wing-down control wheel deflection increased from about 7� to about 200. With regard to engine EPR characteristics at low engine rpm, flight test data obtained during flights conducted between 39,000 and 43,000 feet demonstrate that an increase in recorded and displayed EPR values occurs at low power settings due to inlet spillage over the strut mounted compressor inlet total pressure (PT2) probe.
Between 1013:10 and 1015:06, the Nos. 1, 2, and 3 engines remained at about 1.5 EPR while the No. 4 engine remained at about 1.1 to 1.2 EPR. The airplane continued level at 40,900 feet, but the airspeed continued to decrease at a rate of about 0.25 KIAS/sec. Although the roll angle of the airplane remained fairly constant at about 2.6� to 3.50 left-wing-down, the left-wing-down deflection of the control wheel continued to increase as the indicated airspeed decreased, and, by 1013:43 the deflection had increased to 22.9� the maximum available input from the autopilot. As the airspeed continued to decrease and with the control wheel deflected to, and remaining essentially at, the 22.9� left-wing-down deflection, the airplane began rolling slowly to the right, reaching a wings-level attitude by 1013:58 and then continuing on into a right-wing-down attitude. (See figure 1.)
By 1014:33, the airspeed had decreased to 225 KIAS. Despite the 22� left-wing-down control wheel deflection, the airplane had rolled 23� right-wing-down. (See figure 2.) The airplane's pitch attitude, which until this time had remained constant at 3.1� noseup, now decreased to 1.8� noseup and remained at that angle for about 5 to 6 seconds before returning to the original noseup attitude. During this period, the airspeed increased about 1 KIAS and then began decreasing again. The airplane continued rolling to the right at an increasing rate. In addition, the airplane had begun descending at a rate of about 1,200 feet per minute.
By 1014:50, the airplane had descended to 40,442 feet, the airspeed had decreased to 221 KIAS, and the airplane had rolled and pitched to a 64� right-wing-down and 4� nosedown. (See figure 3.) The 22.9� left-wing-down control wheel deflection had decreased to 200 and, over the next 3 to 4 seconds the control wheel returned to center. In addition, between 1013:06 and 1014:50, the heading had increased from the original 106� heading to 163�.
Between 1014:50 and 1015:23, the DFDR recorded a 10,310-foot descent to 30,132 feet. Between 1014:59 and 1015:06, as the airplane descended from 40,346 feet to 37,102 feet, the recorded data showed a right-wing-down control wheel deflection. The maximum 59� right-wing-down deflection occurred at 1015:00 and then decreased to a right-wing-down deflection which varied between 4� and 16�. At 1015:07, the recorded
data showed a 57� left-wing-down control wheel deflection. During the 10,310 foot descent, the recorded data showed that the airplane's pitch angle decreased to 68� nose-down and then increased back to 11� nosedown. The airplane had rolled over on its back and continued rolling to the right through the wings-level point and to a 25" right-wing-down attitude, essentially completing a full 360� aileron roll. (See figures 4, 5, 6 and 7.) In addition, between 1015:04 and 1015:08, as the airplane was descending, the Nos. 1, 2, and 3 EPRs decreased from about 1.4 EPR to about 1.1 to 1.2 EPR and were at those values when synch was lost on the DFDR at 1015:22. At 1016:06, when synch was restored, the Nos. 1, 2, and 3 engine EPRs were still about 1.1 to 1.2 EPR and remained at those values until 1017:13.
Between 1015:23 and 1017:15, the airplane descended from 30,132 feet to 9,577 feet. During this period, except for some short 3- to 7-second intervals of accurate data, the data recorded by the DFDR were, as stated earlier, either unreliable or erroneous. For example, during the final minute of the descent, the Group 1 synchros were displaying erroneous data. At 1017:13, when the Group 1 synchros began displaying correct data, the airplane was at 9,577 feet and climbing and the airspeed was 221 KIAS. The EPRs on engines 1, 2, and 3 were about 1.23, 1.27, and 1.23, respectively, and increasing, and the thrust increase was accompanied by a 3" left rudder pedal deflection. The number 4 engine EPR was 0.9 and remained constant at that value over the next 40 seconds. While the airplane's altitude remained relatively constant, the indicated airspeed increased slowly until, at 1017:43, the airplane accelerated through 250 KIAS. At 1017:53, the No. 4 engine's EPR began increasing, and, by 1018:12, all four engine EPRs were essentially stabilized at about 1.3 EPR. At 1018:42, Flight 006 requested clearance from Oakland ARTCC to climb.
The lowest indicated airspeeds were recorded between 1016:14 and 1016:22. During this period, speeds between 54 KIAS and 110 KIAS were recorded.
The DFDR data showed that the captain did not introduce any rudder pedal corrections to counteract the asymmetrical forces created by the loss of thrust from the No. 4 engine prior to the loss of control of the airplane.
The maximum vertical acceleration forces recorded during the descent were 4.8Gs and 5.lGs as the airplane descended through 30,552 feet and 19,083 feet, respectively. The 5.1G peak value was recorded on a portion of the tape where data had been lost originally and subsequently recovered, but this value is consistent with the adjacent data which show an arresting of descent rate and a pull-up.
1.12 Wreckage and Impact Information
All the damage found on the airplane occurred during the descent and was caused by aerodynamic overload forces.
Wings and Engine Pylons.--The wings were bent or set permanently 2 to 3 inches upward at the wingtips; however, the set was within the manufacturer's allowable tolerances. The left outboard aileron's upper surface panel was broken and the trailing edge wedge was cracked in several places.
Wing and Body Landing Gear.--The left and right wing landing gear uplock assemblies had separated from their attachment points on the fuselage structure. The interior skin and associated ribs on the left and right wing gear inboard doors were damaged in the vicinity of their striker plates and the striker plates also were damaged.
The doors were damaged in the area where the tires are located when the gears are retracted.
The left and right body landing gear uplock hooks were found in the locked-up position, but the fasteners of their uplock support bracket assemblies had failed at the attach points to the fuselage bulkhead.
The left and right body gear actuator doors had separated, but the forward lateral beams and associated door actuators had remained attached to their respective assemblies, and there were tire marks on the sections of structure attached to the lateral beams. (Note: The uplock assemblies hold the body gear in the retracted position after gear retraction is completed. Except for the body gear tilt assembly, which is pressurized by the No. 1 hydraulic system, the body gear actuators are unpressurized. The tilt assembly is pressurized and remains pressurized so that the body gear wheel bogies can enter or leave their wheel wells without their tires striking the forward wheel well structure.)
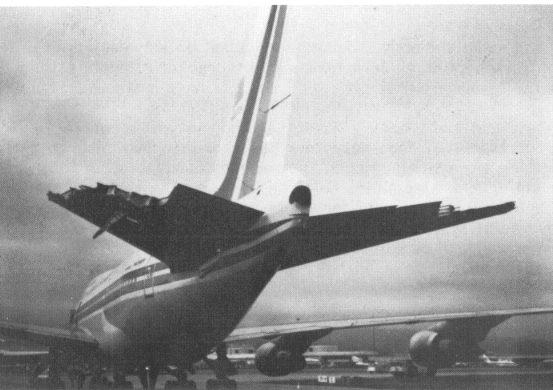
Empennage.--The major damage to the empennage was limited to the Auxiliary Unit APU) compartment, the horizontal stabilizers, and elevators. The APU had separated from its mounts and was resting on the two lower tail cone access doors. The forward side of the APU fire bulkhead appeared to be deflected forward in the area adjacent to the two lower attachment fittings and the two lower support rods had buckled. In the area of the APU, there were several punctures in an outward direction on both sides of the tail cone.
The aft pressure bulkhead was undamaged.
A large part of the left horizontal stabilizer had separated from the remainder of the stabilizer. The separated portion, which began at the outboard tip of the stabilizer, was about 10 to 11 feet long and included the entire left outboard elevator. The hydraulic lines from the No. 1 hydraulic system to the left outboard elevator actuator were severed near the actuator. (See figure 8.)
The right horizontal stabilizer incurred a similar separation. The separated portion included the entire tip of the stabilizer. However, beginning about 5 feet inboard of the tip, the separation moved directly aft to the area of the rear spar and then inboard an additional 5 to 6 feet along the forward edge of the box beam area. The separated portion of the stabilizer included the outboard three-quarters of the outboard right elevator. The hydraulic lines to the outboard elevator actuator remained intact. (See figure 8.)
Powerplants.--Except for some rotational scrubbing on the fan rotor rub strips of the Nos. 1 and 4 engines, none of the four engines were damaged during the accident. A boroscope examination of selected accessible areas of the No. 4 engine's front and rear compressors did not disclose any damaged areas.
1.13 Medical and Pathologica1 Information
Except for the one cabin crew member admitted to a hospital after landing, medical examinations of the flight and cabin crew members were not conducted after the accident nor was toxicological testing of the flightcrew performed.
1.14 Fire
There was no fire.
1.15 Survival Factors
The damage to the passenger cabin was confined to several overhead luggage storage bins and two passenger seats. The seatback at seat 36E was overextended rearward and about 60� aft of upright. When it was brought up to the normal upright position, it would not lock, and fell rearward to the overextended position. The armrest between seats 36D and E was overextended about 60�. It could be raised to the normal up position, but would not go forward to the normal down position. The Safety Board could not determine whether these seats were either assigned to passengers before departure or had been occupied by passengers at the time of the upset. The airplane had 281 seats, 30 of which were not occupied.
The hinges of five storage bins were either sprung or pulled from their mounts and the stops on two bins were missing. Four overhead bins were found open but undamaged.
Two passengers and 10 flight attendants were interviewed, but not all of those interviewed could recall the events of the upset, the descent, and the recovery. Most of those who could recall said that they felt an initial period of moderate negative G forces lasting several seconds followed immediately by a period of stronger positive G forces lasting several seconds. The positive G forces decreased momentarily and was followed by a period of even stronger positive G forces lasting several minutes. Almost all of the interviewees concurred that the initial rolling motion of the airplane was to the right.
1.16 Tests and Research
1.16.1 Powerplants
Upon completion of the visual and boroscope(sic) inspections of the engines, engines No. 1, 2, and 3 were started and the airplane was taxied to San Francisco International Airport's engine run-up area for engine run-up tests. Because the direction of airport traffic would not permit the airplane to be turned into the wind, all of the engine tests were conducted in a prevailing 17-knot tailwind. The evaluation of the data obtained during the run-ups of the engines showed that they were operating within prescribed parameters.
Variable stator vane instrumentation was installed on the No. 4 engine to record the positioning of the variable stator vanes during the run-ups at the airport. The evaluation of the data obtained during the run-up of the No. 4 engine showed the following: N1 (front compressor) and N2 (rear compressor) rotor speeds were normal; at idle thrust, the variable stator vanes were open about 1� to 1.5� above the idle thrust trim point schedule limits; however, at the higher thrust conditions, the subsequent vane positions were within the scheduled trim points. In addition, at the high thrust conditions, the exhaust gas temperature (EGT) was 32�C higher than that produced by a newly refurbished engine at similar high thrust levels. These test data were sent to the manufacturer for a performance evaluation of the No. 4 engine's operational parameters.
On February 27, 1985, the No. 4 engine was removed from the airplane and installed in United Air Line's San Francisco maintenance facility's high bypass ratio turbofan engine test cell and subjected to a calibration check to obtain detailed controlled engine performance and transient operating data. The test cell data were evaluated using the manufacturer's computer generated Module Analysis Program, comparing the obtained test data to baseline data obtained from average JT9D-7A production engines. Although the results of the comparison showed that the performance levels of the No. 4 engine's gas path components were normal for an inservice engine, the transient operating data also indicated that the main fuel control scheduled fuel flow was below expected levels during engine starting; the starting times from light-off to idle were about 25 seconds longer than those of an average JT9D-7A production engine. During engine accelerations above idle, the main fuel control scheduled a fuel flow that was about 200 pounds per hour (pph) toward the lean direction or about 200 pph below expected levels. The engine deceleration time was 0.25 seconds below the minimum acceptable 1.5 seconds and the ground idle speed was about 0.4 percent below the engine's nominal idle trim. In addition, the temperatures supplied to the main fuel control's fuel flow schedule were about 35� F higher than t he nominal input values.
The main fuel control was disassembled to determine the source of the variations from the fuel schedule. Evidence of wear was observed on the throttle valve trimmer knife edge and the mating groove of the multiplying lever. Photographic magnification of the wear areas showed that each of these components was worn about 0.002 inch or a total wear of 0.004 inch. A loss of height (wear) between these two components would have contributed to the change in the main fuel control schedule.
In conclusion, a computer simulation of the engine performance capabilities was conducted using the data obtained during the engine testing and the estimated operating conditions of the airplane at the time of the accident. The simulation showed that if the total estimated air conditioning system bleed air load, coupled with the main fuel control's schedule deviations, were imposed on the engine, the engine would fail to
accelerate or would "hang" at about 76 percent (6,000 rpm) N2 rotor speed. This situation would result in a condition described as "bleed load hogging." During normal engine operation, each engine will supply a proportionate amount of bleed air to the airplane's air conditioning system. If an individual engine remains at or near idle thrust and the remaining engines are operating at higher thrust levels, the engine at or near idle will assume a disproportionate amount of the bleed air load. This bleed load hogging condition raises the engine's "required to run line" and decreases the acceleration rate of the engine. The "required to run line" defines the performance level of an engine in terms of the amount of fuel required to produce a given rpm.
1.16.2 Human Performance Information
The Safety Board examined the relevant operational factors known to affect crew performance. These factors included flightcrew training, flightcrew in-flight duty procedures, and certain behavioral factors which, based on the facts and circumstances, might be relevant to the sequence of events.
Because of the scheduled duration of the flight, 11 hours, an augmented flightcrew was on board. In addition to the three primary flightcrew, an additional fully qualified captain and flight engineer were on board. All five crew members were interviewed by the Human Performance Group concerning their duties, training, and rest periods before and during the flight. (See appendix B.)
The captain had spent 5 days in Jeddah, Saudi Arabia, before returning to Taipei on February 14, 1985; Taipei time is 5 hours ahead of Jeddah time. He was off duty on February 15; on February 16, he flew a 2 hour 30 minute flight to Tokyo, Japan, returning to Taipei (a 3-hour flight) on February 17. According to the captain, during the nights of February 14 through February 17, he went to sleep between 2100 to 2200 Taipei time and awoke about 0700 to 0800. On February 18, he flew a round trip to Nagoya, Japan, and was off duty 15 hours 20 minutes before reporting for duty on February 19.
Flight 006 departed Taipei at 1622 local time and had been airborne about 9 hours 46 minutes when the accident occurred (0214 Taipei time). At the time of the accident, the three primary flightcrew members were on duty. They had been on duty during the takeoff, climb, and initial part of the flight. Thereafter, they each went off duty at intervals ranging from 1 1/2 to 4 hours after takeoff and were replaced by the augmentee flightcrew members, with the captain occupying the first officer's seat during a portion of this period.
The captain was off duty 5 hours during the flight and returned to duty about 2 hours before the accident. During his rest period, the captain slept about 2 hours in the bunk located in the rear of the cockpit. The first officer was off duty about 3 hours during the flight and returned to duty about 3 hours before the accident. The flight engineer was off duty about 5 hours and returned to duty about 2 hours before the accident. The first officer's and flight engineer's activities during their rest periods were not established.
China Airlines Training and Flightcrew Procedures.--China Airlines conducts its own Boeing 747 training using its Phase II simulator and a curriculum developed largely by Boeing.
Although captains and first officers of China Airlines generally fly alternating legs on all airplane types, company policy requires that a captain log 1,000 hours as captain on a particular type airplane before he may permit his first officer to land and take off. Thus, on the Boeing 747, a first officer may only take off and land if the captain assigned to his flight has logged 1,000 hours as captain on the Boeing 747. To compensate for this, the first officers are given additional monthly simulator training to maintain proficiency.
According to China Airlines' chief of flight training and deputy director of flight operations, their first officers are capable of flying the Boeing 747 in any emergency. The China Airlines' Boeing 747 SP Airplane Operating Manual (AOM) Emergency Procedures Section states, in part, that "The captain will take necessary action to establish and/or maintain control of the airplane and call for the appropriate checklist." Thus, according to the flight training chief and operations director, in the event of an unscheduled loss of engine thrust, abnormal engine response to throttle movements, or failure of the engine to respond to throttle inputs, the captain, while primarily directing his attention to flying the airplane, could have directed the first officer and flight engineer to deal with the tasks involved with either restoring full engine performance or shutting down and restarting the engine.
Behavioral Factors: Automation.--The automatic flight systems of the Boeing 747 SP were such that the airplane could be programmed for and was capable of fully automatic flight throughout the entire route. Once the airplane was so programmed, all that was required of the flightcrew was to monitor the progress of the airplane and from time to time update the information required by the airplane's computers. Thus, the flightcrew had been relegated to the role of monitors and had been serving in this role for almost the entire flight until the autopilot was disconnected.
As computers have been added, the pilot's physical workload, as far as physically handling the airplane, has been reduced and, during some phases, eliminated. One researcher has stated that with the addition of computers to the cockpit, the pilot's job is changing from one of manually flying the aircraft to one of supervising computers which are doing navigation, guidance, and energy management calculations as well as automatically flying the aircraft." 8/ The increased automation has not necessarily reduced pilot workload, however, but has shifted it to monitoring tasks which the pilot formerly had to perform, and there is evidence, from both research and accident statistics, that people make poor monitors. For example:
3. In 1979, the flightcrew of an Aeromexico DC-10 stalled the airplane while climbing to cruise altitude over Luxembourg. The crew either intentionally or inadvertently programmed the autopilot for the vertical speed mode rather than the procedurally directed airspeed or Mach command mode. The airplane maintained the programmed climb rate throughout the climb, but at the sacrifice of airspeed. As the climb continued, the engines reached their thrust limit, the thrust available became insufficient to sustain flying speed for that climb rate, and the airplane entered stall buffet. The flightcrew misidentified the intensifying buffet as an abnormal vibration in the No. 3 engine, reduced its thrust, and then shut it down. The airplane stalled, rolled to the right, and the recovery maneuver was executed successfully after an altitude loss of about 11,000 feet. The Safety Board found that "the flightcrew was distracted or inattentive to the pitch attitude and airspeed changes as the airplane approached the stall." 12/
Research also indicates that the excursion from a stabilized condition might be exaggerated even after a system anomaly is detected, because of the period required for a pilot to transition from system monitor mode to system controller. Time is needed to "ascertain the current status of the airplane and assess the situation," 13/ before the pilot can reenter the control loop and take corrective action.
In addition, accident investigations have also indicated a reluctance on the part of the flightcrews to disconnect an automated flight system and take manual control of the airplane even though the automated system in question may be operating outside of system limitations or will not accept or maintain programmed inputs. In cases involving two runway overruns after landing, the flightcrews continued to use the autothrottle speed control systems (ATSC) during the approaches even though the indicated airspeeds provided by the ATSCs were well above the calculated approach speeds that the flightcrews had inserted into the systems. In one accident, the Safety Board found that one of the causal factors was the captain's "decision to accept and maintain an excessive airspeed derived from the autothrottle speed control system during the landing approach
which caused the airplane to land about 2,800 feet beyond the runway's displaced threshold." 14 /. In the other accident, the Safety Board found that one of the causal factors of the accident was the "over reliance on the autothrottle speed control system which has a history of recent malfunctions." 15/
As a result of that investigation, the Safety Board issued Safety Recommendation A-84-123, on November 15, 1984, urging the FAA to:
The Safety Board has classified the FAA's response to this recommendation as "Open--Acceptable Action," pending completion of the FAA's actions on this issue.
Behavioral Factors: Monotony and Fatigue Research has also been conducted to examine the effects of prolonged monotony and boredom on human performance. O'Hanlan, in a review of the literature, noted:
Smith, in a review similar to O'Hanlan's but based on somewhat different literature reached similar conclusions. He:
O'Hanlan concluded that:
Related to the above is a considerable body of research 18/ and 19/ which outlines the cyclical nature of many of the physiological processes in humans, including sleep-wake cycles, urinary excretion, and body temperature. These cycles, which are collectively known as circadian rhythms for their daily periodicity, exert a strong but often suble(sic) influence on human performance capabilities. Disturbance of these circadian rhythms occurs among shiftworkers, for example, who must work during the daytime on some days and at night on others, in a irregular manner. In addition, jet travelers flying east-west or transmeridian, feel the effects since they often arrive at their destination at a local time that is several hours different than the one their circadian rhythms are maintaining. As a result, researchers have noted 20/ that:
This can produce fatigue in addition to the fatigue normally associated with extended waking periods experienced by the transmeridian traveler.
1.17 Other Information
1.17.1 Airplane A.C. Electrical System
Primary a.c. electrical power is supplied to the airplane's a.c. buses by four engine driven generators monitored and controlled from the flight engineer's instrument panel. Each generator powers its a.c. bus through its generator breaker; closing the generator breaker switch on the flight, engineer's instrument panel closes the generator breaker and connects the generator to its a.c. bus. The four generator a.c. buses are paralleled on the synchronizing (synch) bus by four bus tie breakers. During normal operation, the four bus tie breakers are closed and the generators are operated in parallel.
Each generator is driven by its engine through a constant speed drive (CSD). If a generator's CSD falls below operating speed (underspeed), the generator breaker will open and disconnect (trip) the generator from its a.c. bus. In this case, the bus tie breaker should remain closed, or, if automatically opened (tripped), it will reclose automatically after the generator breaker has opened and the generator's a.c. bus will be powered by the synch bus. An underspeed trip occurs whenever the rotation of an engine's rear or high speed compressor (N2) drops to or below 42 percent. The Pratt and Whitney JT9D-7A engine "In-flight Restart Envelope" chart shows that at 35,000 feet and 304 KIAS, a windmilling engine 21/ would only develop N2 rotation speeds of about 31 to 32 percent; at 24,000 feet and 384 KIAS a windmilling engine would develop N2 rotation of about 33 to 35 percent. Higher N2 rotation speeds would require indicated airspeeds well in excess of the airplane's Vmo. According to Boeing personnel, a generator could not be supported by a wind milling engine.
The DFDR drive and transponders are powered by the airplane's essential a.c. bus. Dependent on the positioning of a rotary selector switch on the flight engineer's instrument panel, the essential a.c. bus can be powered by the No. 4 generator a.c. bus or directly by any of the other three generators. However, during normal operation, the selector switch is placed in the "normal" position and the essential a.c. bus is powered by the No. 4 generator's a.c. bus. At the time of the in-flight upset, according to the flight engineer, the essential bus selector switch was at the "normal" position and he did not move it either before, during, or after the upset.
1.17.2 Automatic Flight Systems
Two automatic flight systems were engaged when the in-flight upset occurred: the PMS and the autopilot.
The Performance Management System, when coupled to the autopilot, provides ' pitch steering inputs to the airplane's pitch control system. The PMS also provides thrust control for the climb, cruise, and descent flight modes above 2,500 feet above ground level (AGL) to maintain pilot selected altitudes and speeds. When the PMS is selected, control of the autothrottle servomotor is switched from the Full Flight Regime Autothrottle System (FFRATS) computer to the PMS computer. The flight modes are pilot selected: automatic transitions at top-of-climb, top-of-descent, and bottom-of-descent may be pilot armed. The control is based on pilot loaded information, ambient conditions, and the system performance database optimized for minimum fuel consumption, within operational constraints, including computed engine thrust limits and speed envelope. The system also stores up to 36 navigational waypoints (fixes), and, when given waypoint control, it will transmit waypoint data to the Inertial Navigation System (INS), which is interfaced through the autopilot to the airplane's lateral flight controls.
When the autopilot is engaged, the PMS can be coupled to it by placing the autopilot's speed mode selector switch in the "PMS" position; however, the PMS cannot be coupled to either the autopilot or the autothrottle servomotor below 2,500 (AGL). Since the PMS computer is programmed to provide the most fuel-efficient speeds and altitudes, China Airlines' flightcrews are encouraged to use the PMS to minimize fuel consumption.
The Boeing 747 SP is equipped with two autopilots; however, except in autoland mode, only one autopilot is used to control flight. The autopilot engage switch, located on the Autopilot/Flight Director (AP/FD) Mode Selector panel above the center instrument panel, has two control positions: manual and command. Navigational control inputs to the autopilot from the airplane's navigational radios, INS and PMS, are only possible when the engage switch is in the "command" position.
Altitude hold capability is available in both manual and command modes of the autopilot, but the altitude mode switch is off for PMS operation. PMS altitude is controlled by the altitude selector on the AP/FD mode selector panel. The PMS will command a level off at the altitude inserted in the altitude selector (ALT SEL) counter on the AP/FD Mode Selector panel.
Rotating the autopilot's speed mode selector switch located on the AP/FD mode selector panel from "PMS" to "OFF" releases the autopilot from the PMS mode. With the speed mode selector switch in the "OFF" position and the altitude hold switch off, the pilot can vary the airplane's attitude by rotating the pitch control wheel on the autopilot manual control module in the desired direction. (The manual control module is on the aisle stand between the pilots' seats.)
As stated earlier, the autopilot uses only the airplane's ailerons (inboard and outboard) and spoilers for lateral control; rudder and rudder trim are not used for this purpose. The lateral control available to the autopilot is equivalent to about 22� of control wheel deflection. Flight spoiler actuation begins at 11� of control wheel travel. The outboard ailerons are "locked" in the faired positions at the higher speeds and do not unlock until below about 230 KIAS.
1.17.3 JT9D-7A Engine Operating Procedures
Procedures describing all phases of the operation of the JT9D-7A engine are contained in China Airlines Airplane Operating Manual (AOM). Procedures dealing with an unscheduled thrust loss, an abnormal response to throttle advancement, or a "hung" or "slow engine acceleration" [N2 below 80 percent, EGT normal], and single engine shutdown are described in the Alternate Operations part of the AOM's powerplant section. In-flight engine start procedures are described in the Emergency and Abnormal Procedures section of the AOM.
According to the AOM, emergency procedures are "those where immediate and precise action on the part of the crew in a foreseeable but unusual situation will substantially reduce the possibility of personnel injury or loss of life;" abnormal procedures are "those 'irregularities' that require the use of a checklist;" and alternate operations are "procedures that are designed to cope with 'irregularities' that are not included on the Emergency/Abnormal Checklist, but are available for reference." The AOM further defines alternate operations, stating, in part, "A crew member detecting an existing or impending condition requiring the use of Alternate Operational Procedures will inform the Captain. On the Captain's command, the responsible crew member will perform the procedure and advise the Captain of the completion and system status. Alternate Operational Procedures may be performed by recall or references; also, they may be reviewed by the crew member prior to the accomplishment of the procedure." A few alternate operations require immediate action and must be accomplished by recall, but none of these include the engine operations described above.
The alternate procedures dealing with loss of engine thrust, abnormal responses to throttle movements, slow acceleration, etc., are designed to restore normal engine operation and prevent either an engine shutdown or flameout. The procedures also contain engine operating and EGT limits within which the engine must operate during its recovery. If these limits are exceeded, the flightcrew must place the fuel start lever in "cutoff" and shut the engine down. (See appendix D.)
In-flight start procedures are described in the AOM's Emergency and Abnormal Procedures section. Only the "Multiple Engine Shutdown/Restart" procedure is classified as an emergency procedure and encased in a black border. The first two steps of the procedure require the main boost pump switches and standby ignition switches to be turned on; thereafter, the procedure describes the remaining steps required to restore the engine. (See appendix D.)
The In-flight Start Procedure is not encased in a black border; therefore, it is an abnormal, not an emergency, procedure. (See Appendix D.) The procedure indicates that a windmill start can be made at airspeeds above 250 KIAS; below 250 KIAS, the ignition switches must be placed in ground start to direct engine bleed air to the pneumatic starter to assist compressor rotation during the restart. The JT9D-7A engine In-flight Restart Envelope Chart indicates that 30,000 feet is the maximum altitude at which a successful restart can be expected.
The engine emergency and abnormal procedures designate which flightcrew member is to perform the required tasks (appendix D). Examination of these procedures show that the first officer does not have any assigned tasks.
1.17.4 Engine-out Training and Flight Procedures
The captain completed his initial Boeing 747 training at the Boeing Company's training facility in Seattle, Washington on May 7, 1980. The training curriculum included ground school, simulator training, flight training, and his successful initial airplane rating check. The required flight maneuvers and the recommended pilot techniques for accomplishing these maneuvers are described in the Boeing Company's Boeing 747 Training Manual (TM), a copy of which is given to each student receiving training at the company's Seattle facility.
The pilot techniques required to counteract efficiently the loss of thrust from an engine are described in the TM's Engine Out Familiarization section. The TM states, in part, that the airplane's response to an in-flight engine failure will be an almost simultaneous "yaw and roll toward the failed engine. In instrument flight conditions, roll (resulting from yaw) is usually the first airplane response." With regard to pilot reaction, the TM states, "Any engine failure should trigger the same sequence of thought and action. Apply rudder (and aileron if required) to counter thrust asymmetry, control flight path and airspeed, and then accomplish the appropriate engine failure procedure after the airplane is stabilized..
The TM also describes the techniques to use if the engine is lost with the autopilot engaged. The TM states, in part, "If an engine failure occurs with the autopilot engaged, add thrust and trim the rudder to approximately center the control wheel. Disengage the autopilot and follow the trim procedure under Yaw and Roll Control, this section. Reengage the autopilot." The TM also cautions that, "It is good procedure to always have a firm hold on the controls when the autopilot is disengaged."
The procedures contained in the Yaw and Roll Control section of the TM describe the amount of rudder and roll control available to counteract the effects of asymmetric thrust and the most efficient way to apply these corrective control inputs. The TM states, in part, that when
the rudder input is correct, very little control wheel displacement or lateral trim is necessary. Refine the rudder input as required and trim the rudder so the control wheel remains approximately level. To hold the wings level, a small wheel input away from the failed engine is required due to the rolling movement generated by the larger rudder deflections associated with engine out trim. The rudder required to trim the airplane with a failed outboard engine and the other three engines at MCT (maximum continuous thrust) is within rudder trim authority.
The captain of Flight 006 stated that he had never experienced an engine failure during flight, although he had received engine-out training in the simulator. His training record showed that, in addition to the mandatory loss of engine-thrust after takeoff maneuver required during his recurrent simulator training checks, he had demonstrated his ability to cope with an in-flight engine failure or shutdown during his initial training on 11 of his simulator training flights.
The "Air Work" portion of the China Airlines Boeing 747 simulator curriculum requires pilots to demonstrate proficiency in the following maneuvers: steep turns, stall recovery, and maneuvers at minimum airspeeds. Recovery from unusual attitudes is neither required nor administered. A survey of the simulator curricula of the major U.S. air carriers showed that the "Air Work" portion of their simulator curricula for their wide bodied jet aircraft is similar to that of China Airlines. The captain's training records showed that he had demonstrated his ability to cope with the "Air Work" maneuvers satisfactorily.
1.17.5 Actions Taken by the Additional Flightcrew Members
The relief flight engineer and captain were resting in the bunks at the rear of the flight deck when the sequence of events leading to the upset began. The relief flight engineer said that he heard a "tapping sound" through the aircraft structure, opened the curtains, and asked if anything was wrong. He said that this was about the time the primary flight engineer had discovered that the No. 4 engine had "flamed out" and "I saw him trying to restart it but in vain." He said that the first officer told him "to come forward and help start the No. 4 engine," and he moved forward.
According to the relief flight engineer, the primary flight engineer was turning the standby ignition switch on when he reached the area behind the flight engineer's seat. He said that he had felt "a little slip in the aircraft," but he felt that the captain was correcting the situation although the airplane had entered a slight right bank. He saw the flight instruments briefly and "noted that the aircraft was leaving FL 410 with a six to seven hundred foot per minute rate of descent." Thereafter, he was thrown back into the rear jump seat by strong G forces.
The relief flight engineer said that he felt two periods of heavy G forces, separated by a "short period of lighter forces." During the periods of heavy G forces, he was unable to move to the front to help the primary flight engineer with the engines. According to the relief flight engineer, during the dive he "saw only the number 4 generator breaker (open) and CSD (constant speed drive) lights on, and heard no other warnings. I felt no buffeting or shaking in the aircraft." The relief flight engineer's description of the ADIs' portrayals was identical to those of the primary flightcrew. He said that he did not see any fuel cutoff levers moved to "OFF" at any time.
During the dive, he saw the primary flight engineer move the Nos. 1, 2, and 3 throttles forward twice, but there was no response on the engine gauges. He said, "I was able to reach forward once during the lighter [G] force period and moved the throttles forward once, again with no response."
As the airplane recovered from the dive, the relief flight engineer said that he helped the primary flight engineer turn on the standby ignition and power was restored on engines Nos. 1, 2, and 3.
The relief captain first became aware of the situation when he heard the primary flight engineer announce that the No. 4 engine had flamed out and that the first officer, almost simultaneously with the "flame out" announcement, asked the relief flight engineer to come forward and help restart the engine.
The relief captain said that he climbed out of his bunk after the relief flight engineer had started forward. At that time he could not see the flight instruments or any outside visual references. The relief captain said that while he was trying to move
forward to help, "strong G forces threw me to the floor.... All during the descent, the G forces were so strong that I could not rise up or move until the aircraft had recovered. I then went forward to check the engines but everything was normal by that time."
The flightcrew members of Flight 006 were certificated properly and were qualified for the flight. There was no evidence that their performance was affected by medical problems. Although there were writeups relating to the loss of thrust on the No. 4 engine on the two previous flights, there was no evidence of any preexisting maintenance discrepancies that could have contributed to the accident. The facts showed that the airplane had been maintained in accordance with all applicable regulations and company requirements.
Based upon the winds and temperatures reported in the area of the accident, Flight 006 was flying in the polar jet stream just west of the centerline of a trough on the leading edge of a jet stream maxima, and between a divided tropopause. Within an atmospheric structure like this, there would have been strong horizontal and vertical wind shears and possible clear air turbulence. Based on the consistency of the temperatures reported by other airplanes operating in the area, it is doubtful that there were significant temperature variations. Since the flight encountered clear air turbulence of sufficient magnitude to require the captain to turn the "fasten seatbelt" light on, the Safety Board concludes that the airspeed variations requiring the throttle adjustments before the accident were caused by wind shear associated with the turbulence.
The flightcrew's statements about the ADIs failing were not substantiated by the facts. It is most likely that the flightcrew became spatially disoriented during the upset. They were unable to believe the information displayed on the ADIs, did not recognize the unusual attitude of the airplane, and were unable to take the correct action to recover the airplane until it began to emerge from the clouds.
Although the captain said that the airplane exceeded Vmo twice and also decelerated below 100 KIAS during the dive, all three crew members said that they did not hear the overspeed warning and that the stall warning stickshaker did not activate. Examination of the reliable recorded airspeed data points showed that the Vmo limitation was not exceeded during the descent. However, the recorder data does show airspeeds at or below 100 KIAS. The Safety Board cannot explain why the stall warning stickshaker did not activate, or if it did activate, why it was not felt or heard by the flightcrew.
The Safety Board's investigation and analysis concentrated primarily on two major areas. First, the investigation sought to identify the cause of the loss of thrust on the No. 4 engine, and thereafter to assess whether the actions taken by the flightcrew to cope with the malfunction were reasonable and proper. Second, the investigation sought to determine why the flightcrew was unable to maintain control of the airplane after the loss of thrust on the No. 4 engine.
2.1 Ihe Engine Failure
About 1010:46, the PMS, in response to the increased airspeed caused by the wind shear, had decreased the EPRs on all four engines to 0.9 EPR. Then, about 1011:10, the PMS, in response to the now reduced airspeed, began to advance the four throttles to restore the airplane to the commanded 0.85M. The investigation of the No. 4 engine and its components showed that it had experienced a lean shift of the acceleration schedule
resulting in a reduction in the fuel flow available for engine acceleration. A reduction of this type reduces the rate at which the engine would accelerate from flight idle. The DFDR data showed that all four engines started to accelerate; however, the data also showed that the No. 4 engine accelerated at a slower rate than the others. As engines Nos. 1, 2, and 3 accelerated, their respective bleed air controllers closed their 15th stage or high stage bleed air valves. Since the No. 4 engine accelerated slower than the other engines, it did not achieve high enough power for its bleed air controller to close the high stage bleed valve at the same time the high stage bleed air valves were closed on the other engines, and the No. 4 engine, at high altitude, probably assumed most of the air conditioning air bleed load. The additional fuel demand imposed by the "bleed load hogging," in combination with the reduced fuel flow available because of the control lean shift, caused the No. 4 engine to fail to accelerate and to "hang" at slightly above 1.0 EPR.
The flight engineer stated that he moved the No. 4 throttle to idle and then advanced it slowly, trying to restore the engine to normal operation. However, the procedure for restoring a "hung" engine to normal operation also required the flight engineer to close the No. 4 engine's bleed air valve (see appendix D), and this he did not do. Closing the bleed air valve shuts the high stage bleed air valve and reduces the engine's bleed air load supply requirements. However, given the altitude at which the airplane was flying, and the fact that the flight engineers on two previous flights were unable to restore the engine to power under similar circumstances, the Board cannot state that the flight engineer would have been able to restore the engine to normal operation even had he closed the bleed air valve. Since the DFDR showed that the No. 4 engine did not accelerate with the other engines and remained at about 1.0 EPR until it fell below that EPR value at 1012:42, the Safety Board concludes that the No. 4 engine had not flamed out initially, but had "hung."
At some indeterminate time thereafter, the flight engineer decided that the No. 4 engine had flamed out and informed the captain. Between 1012:42 and 1013:04, the No. 4 engine EPR dropped from 1.0 to about 0.7 EPR. By about 1013:09, the No. 4 engine EPR had returned to about 1.0. Based on these data, and the fact that the flight engineer said that he had not moved the engine start lever to cutoff, the Safety Board concludes that engine No. 4 did flame out about 1012:42 and began to decelerate toward windmilling rpm; the subsequent increase in the EPR was caused by inlet spillage from the windmilling engine over the PT2 pressure probe on the strut. The restart attempt was unsuccessful because the attempt was made well above the altitude limits of the inflight airstart envelope.
About the time that the airplane was entering an unusual attitude, but before the G forces rendered him immobile, the flight engineer stated that the other three engines had lost thrust. He advanced the throttles, but said that the engines did not respond. He then placed the standby ignition switch on, and sometime after that he was pinned to the aisle stand by G forces.
The Safety Board believes that the Nos. 1, 2, and 3 engines had not flamed out and that the low engine parameters observed by the flight engineer resulted from the throttles being at or near idle. Advancing the throttles at this point would have produced an engine acceleration which was much slower than would be observed at sea level because the acceleration fuel schedules are biased by total air temperature. Based on the flight engineer's description, he must have observed the Nos. 1, 2, and 3 engines and manipulated their throttles somewhere above 30,000 feet; the cold temperatures existing at these altitudes will result in lower acceleration fuel flow available and a lower acceleration
rate. In addition, the airplane's changing attitudes, the maneuvers it was undergoing, and the resultant high G forces may have compromised the engineer's ability to conduct a proper and thorough scan of the applicable engine instruments.
The DFDR data indicates that the flight engineer's recollection of the time at which he placed the engine ignition to standby was not accurate. The flight engineer stated he did this right after he had decided that engines Nos. 1, 2, and 3 had lost thrust. Thereafter, he said, he was rendered immobile by G forces and was forced down against the aisle stand. At 10,000 feet and about the time that the captain said that he saw the horizon outside the airplane, he said that he again "hit the standby ignition; Nos. 1, 2, 3, started, No. 4 did not." The DFDR data showed that the Group 1 DFDR synchros were lost for about a 5-second period beginning about 1016:08, indicating that standby ignition had been selected at that time. From 1016:14 to 1016:22, the Group 1 synchros recorded accurate data, indicating that standby ignition was off. During that 8-second period, the airplane descended from 14,541 feet to 13,950 feet and the airspeed increased from 87 KIAS to 110 KIAS. >From 1016:23 to 1017:12, the Group 1 synchros were lost again, indicating that standby ignition had been reselected again. During this period, at about 1016:41, the Nos. 1, 2, and 3 EPRs began increasing. At 1017:13, when the Group 1 synchros were restored, the airplane was at 9,577 feet, at 221 KIAS, and in fairly stable flight. The EPRs on engines Nos. 1, 2, and 3 had increased from about 1.01 to 1.23 and were continuing to increase. Since the captain was decreasing the descent rate during this time and was allowing the airplane to accelerate smoothly, the Safety Board believes that it was highly unlikely that the airplane ever achieved the necessary 250 KIAS to permit a successful airstart on engines Nos. 1, 2, and 3 and that, in fact, they had not flamed out.
The contention that engines Nos. 1, 2 and 3, did not flame out is further supported by the following:
While there can be little doubt that the loss of thrust on the No. 4 engine was the precipitating factor of the accident sequence, the loss of one engine, albeit an outboard engine, during high altitude cruise should not cause an experienced flightcrew to lose control of their airplane. Indeed, the Airline Operating Manual does not even classify this mishap as an emergency procedure. Therefore, the Safety Board directed its attention to the reasons why the flightcrew was unable to maintain control of the airplane after the loss of thrust on the No. 4 engine.
2.2 The Flightcrew
Although the facts developed during the investigation showed conclusively that the accident occurred because the captain failed to maintain control of the airplane after the loss of thrust on the No.4 engine, the Safety Board also sought to determine the reasons that may have led to the captain's inability or failure to employ the procedures that would have prevented this from happening. Therefore, in its analysis, the Safety Board evaluated data contained in past reports of similar accidents, as well as psychological literature discussing the factors that contribute to breakdowns in decision making and monitoring capability. These areas included boredom, monotonous environmental conditions, fatigue due to circadian desynchronosis, and over-reliance on automated flight systems. In addition, the manner in which the first officer and flight engineer performed during the loss of control sequence was also evaluated in relation to the above areas.
Although the first officer was capable of either flying the airplane or assisting the flight engineer in his analysis of the loss of thrust on the No. 4 engine, the captain did not task him specifially with either chore. During this period, the additional task levied on the first officer was to obtain clearance from Oakland ARTCC to descend, and the captain did not direct the first officer to obtain an emergency descent clearance. The facts showed that the first officer performed his communications duties in a timely manner; that he had warned the captain of the decreasing airspeed and the increasing right bank; that after the No. 4 engine flamed out he had, without informing the captain, instructed the relief flight engineer to come forward and help the flight engineer restart the No. 4 engine; and that he came to the captain's assistance on the flight controls without being instructed to do so. Although the first officer was subject to fatigue, boredom, and the same monotonous environment as the rest of the crew, and although he had less off-duty time during the flight than the captain and flight engineer, he seemed to have performed his assigned duties and overall monitoring tasks in a timely manner. Given these factors, the Safety Board cannot state with any confidence that any of the psychological factors that could have reduced his capability to perform affected his actions during the accident sequence. The facts, limited as they are, indicate that his performance was unaffected by these factors.
With regard to the captain and flight engineer, both men were performing in a time spectrum that was later than their typical sleep periods. Although both men had taken a 5-hour rest during the flight, the quality of their rest during this period cannot be equated to that which would have been achieved by sleep either at home or in a hotel. Their duty tasks consisted of routine monitoring of the performance of the airplane's automated flight systems, a task that is repetitive and monotonous and capable of producing a state of boredom. The existence of these conditions required the Safety Board to examine the possibility that they might have influenced and derogated the manner in which the flight engineer and captain performed during the emergency.
The flight engineer's performance before, during, and after the loss of control disclosed actions that were correct and timely and other actions that deviated from the required checklist procedure or that demonstrated that he had been unable to analyze correctly the portrayal of the airplane's engine instruments. During the 1 minute 20 second period between the inception of the "hung" engine and the flameout, the flight engineer informed the captain of the status of the engine, moved the throttle aft, then moved it forward to align with the other throttles and awaited the results of the procedure. Since the procedure requires the throttle to be moved slowly and also incorporates a time to interval to wait and evaluate the engine response, the 1 minute and 20 seconds required to accomplish the task, evaluate the engine response with the captain,
and then decide that the engine had either flamed out or had flamed out during his efforts to restore the engine to normal performance were correct and appear to be timely. The facts showed that the flight engineer did not review the alternate operations procedure for this malfunction before trying to restore the engine; however, the AOM states that this procedure may be performed "by recall or references," and also that the AOM may be reviewed before accomplishing the procedure. As a result, the flight engineer did not recall that he was required to close the bleed air valve before manipulating the throttle.
After the flight engineer told the captain that the No. 4 engine had flamed out, the captain ordered him to restart the engine. The flight engineer, without referring to the checklist, placed the second ignition system of the No. 4 engine to the "flight start" position, thus providing continuous ignition from both igniters to the engine's chambers. This action was required by the applicable checklist procedure.
During the descent, the flight engineer had concluded erroneously that the other three engines had flamed out. Several factors led to this misdiagnosis. Shortly after the upset, engines Nos. 1, 2, and 3 were reduced to flight idle thrust. The flight engineer did not move these throttles; thus, when he saw the engine instruments during the dive, the EPRs on engines Nos. 1, 2, and 3 had decreased from their cruise thrust of about 1.5 EPR to flight idle and were nearly aligned with that of the No. 4 engine, which he knew had flamed out. The failure of these three engines to respond to throttle movements would also tend to indicate that the Nos. 1, 2, and 3 engines had flamed out. Since he had observed that the No. 4 generator was off the line as a result of the flameout of the No. 4 engine, the fact that the airplane still had a.c. electrical power should have alerted him to the possibility that the remaining engines had not flamed out, certainly not all of the remaining engines. Perhaps the flight engineer should have checked the generator panel; however, when the upset occurred, he was facing forward and trying to evaluate the thrust readings. The electrical panel would have been 2 to 3 feet to the right and slightly aft of him. During the dive, the flight engineer's face was pressed into the center aisle stand by the "G" forces; thus, any attempt to see the electrical panel would have been somewhat difficult. However, having reached this erroneous conclusion, his next action, albeit based on the erroneous conclusion, was timely and was required by the Multiple Engine Shutdown/Failure emergency checklist; he turned on the standby ignition switch.
The evaluation of the flight engineer's performance shows that for the most part, his actions were timely and correct; however, he forgot to close the engine bleed valve switch and he was not able to evaluate correctly the operational status of engines Nos. 1, 2, and 3. These deviations from checklist procedures and the inability to evaluate the status of engines Nos. 1, 2, and 3 correctly could be attributable to any one, or all, of the following factors: a lack of knowledge of the airplane systems and procedures; the traumatic effect of the upset and subsequent descent on the flight engineer's ability to scan the center and flight engineer's instrument panels closely and accurately; and the deleterious effects of fatigue resulting from the combination of monotony and boredom, circadian desynchronis, which affected the flight engineer's ability to monitor his instruments properly, to obtain all the available data in a timely manner, and to analyze these data accurately. Based on the flight engineer's performance of his duties, the Safety Board can find little if any evidence to support a conclusion that the effects of monotony, boredom, and fatigue impaired the flight engineer's performance of his duties. The Safety Board concluded that a preponderance of the evidence showed that the deviations and omissions noted above resulted from either a lack of knowledge of the airplane systems and procedures, the traumatic effects of the upset and subsequent descent on the flight engineer's ability to scan his instrument panels, or a combination of these two factors.
In the event of an abnormal flight condition, company policy and the AOM dictated that the captain assume control of the airplane and direct the other crew members to deal with the abnormal condition. Since the captain was at the controls when the flight engineer told him that the No. 4 engine did not accelerate, there was no need for him to take any further action other than to monitor the flight engineer's attempts to analyze the engine's performance and restore it to normal operation. He did not disengage the autopilot since it relegated the tasks involved with flying the airplane to merely monitoring the autopilot's performance. Had he disengaged the autopilot, as recommended in his training, he would have been required to perform the physical, more difficult, and more time and attention consuming tasks involved with flying the airplane manually.
The effects of the asymmetrical thrust condition began to assert themselves at about 1011:10, and the No. 4 engine flamed out about 1012:42. Based on the decrease in pitch attitude and the subsequent momentary airspeed increase, the Safety Board concludes that the the PMS was disengaged about 1014:30. Based on the initial movements of the control wheel from its 22.9� left-wing-down position, the Safety Board also concludes that the autopilot was not disengaged until 1014:50. During the 3 minute 40 second period of deceleration, the statements of the captain and flight engineer showed that the captain was totally cognizant of the engine situation, and thereafter, his attention appeared to focus almost exclusively on the airplane's decreasing airspeed. According to the captain, he had disengaged the' autopilot in order to lower the nose of the airplane faster and recover airspeed. Although he said that he was aware that the airplane had entered a right bank, he was apparently not aware of the magnitude of the right-wing-down attitude.
The Safety Board concludes that one of the causal factors of the accident was the captain's reliance on the autopilot while the airplane was decelerating. During this 3 minute 40 second period, the captain allowed himself to remain removed from the "control loop" by leaving the autopilot engaged. As a result, he was not aware of the increasing control inputs required to maintain level flight. Had the captain placed himself in a "hands on" relationship with the airplane by disconnecting the autopilot at the onset of the engine problem, he probably would have been more alert to the increasing asymmetrical forces being exerted on the airplane since he would have been required to make the necessary control inputs to maintain level flight. Since he had no physical relationship with the airplane flight controls, the only cues available to him to monitor the airplane's attitude and performance were the visual cues available from either the airplane instruments or the outside horizon since the airplane was flying above the clouds. However, even under conditions of visual flight, the flight instruments remain the primary tools at high altitudes for maintaining level, stabilized flight in large airplanes. The captain's statement corroborated the fact that he was relying on these instruments for that purpose. Under these conditions, therefore, the primary instrument for attitude control was the attitude director indicator, which may not have concerned the captain initially since it depicted either a wings-level attitude or a very slight left-wing-down bank. With regard to heading, over the period between 1011:09 to about 1014:00, the heading increased about 4�, a change so slight as to be almost imperceptible. Thus, except for airspeed, which concerned the captain greatly, the only thing in the cockpit that would have depicted the worsening control situation was the control wheel's increasing leftwing-down deflection. However, this was an area which was not included in the captain's regular instrument scan pattern, and since he was not "hands on," he was not aware of the deflection.
During the latter part of this period, the captain's statement indicated that his attention seemed to be directed almost solely to the airspeed indicator as he tried to arrest the airspeed decrease. Thus, when he failed to arrest the decrease by disengaging the PMS and lowering the airplane's nose by rotating the pitch control wheel on the autopilot manual control module, he disconnected the autopilot.
As noted earlier, an excursion from a stabilized condition might be exaggerated during the transfer from system monitor mode to system controller because time is needed to ascertain the status of the airplane and assess the situation before the pilot can reenter the control loop and take corrective action. When the autopilot was disengaged, the airplane's excursion from the stabilized condition was well advanced and at the point where immediate and proper corrective action was required if the situation was to be remedied safely. The captain was not only unable to assess the situation properly, he was confused by it; therefore, he was unable to take the necessary action to correct the situation. The DFDR data indicated that his actions most probably aggravated the situation. The Safety Board concludes that the captain became spatially disoriented at the onset of the upset and was unable to reorient himself until the airplane began to emerge from the clouds. The fact that the first officer was unable to help the captain reorient himself during the descent showed that he also became disoriented during the upset and descent.
The Safety Board further notes that the captain did not, as was recommended during his training and in his training manual, disengage the autopilot when the No. 4 engine initially "hung." Thereafter, he relied on the autopilot to maintain the airplane in straight and level flight during the deceleration, and he did not apply left rudder trim to level the control wheel before disengaging the autopilot. Since the decreasing airspeed was initially and readily apparent and would, if allowed to continue unchecked at FL 410, seriously menace the safety of his airplane, the captain's continuing preoccupation with airspeed control was understandable. However, the captain was an experienced multiengine and Boeing 747 pilot and he also should have known how the loss of thrust from an outboard engine would affect an airplane's controllability, especially when it is coupled with decreasing airspeed. Given his Boeing 747 experience, the captain should have also known that the autopilot's lateral control authority did not include the rudder and that the effects of the thrust loss could only be counteracted by introducing a left-wing-down roll, an action which would also introduce a side slip, increase drag, and aggravate the airspeed decrease. Given these circumstances, the Safety Board explored the reasons why the captain was not alert to this condition and why he was not monitoring his attitude direction indicator more closely during this phase of the operation. Had he done so, he would have noted the airplane was rolling right-wing-down, that the autopilot could no longer maintain the airplane's heading and roll attitude, and that additional control inputs were required, i.e., rudder or rudder trim. The DFDR readout showed that after the No. 4 engine had "hung," the airplane accelerated to about 250 KIAS and stabilized at that airspeed for about 1 minute 30 seconds. During this period, the autopilot maintained the airplane at a relatively wings-level attitude with left-wing-down control wheel deflections of about 6� to 10�. The full effects of asymmetrical thrust were not felt until after the No. 4 engine flamed out. Thereafter, the airplane began to decelerate, its rate of deceleration began to increase, and the captain's statement showed that his attention began to focus almost exclusively on the airplane's airspeed. When the captain disconnected the PMS from the autopilot, the airplane was rolling through the 20� right-wing-down attitude and the evidence showed that the captain did not observe the airplane's roll attitude. After disengaging the PMS and inserting a nose-down control correction into the autopilot, the captain continued to monitor the airspeed indicator to
observe the results of the nose-down control correction. During this period, the airplane continued to roll to the right and past the 45� right-wing-down attitude. Although the ADI is to the right of and abuts on the airspeed indicator, the captain never noticed the right-wing-down ADI indications until he disconnected the autopilot. The evidence showed that, starting just before he disconnected the PMS, the captain was distracted by the decreasing airspeed. With the continuing decrease, the captain's distraction with the airspeed increased to the point where his instrument scan pattern broke down and his visual attention became fixed on the airspeed indicator. The ADI went unobserved. The Safety Board can only conclude that the captain was distracted first by the evaluation of the engine malfunction and second by his attempts to arrest the decreasing airspeed, and that, because of these distractions, he was unable to assess properly and promptly the approaching loss of airplane control. The Safety Board also concludes that the captain over-relied on the autopilot and that this was also causal to the accident since the autopilot effectively masked the approaching onset of the loss of control of the airplane.
Although the Safety Board has cited distraction and over-reliance on the autopilot as causal factors, it also notes that the airplane had been airborne about 10 hours, that it had traversed several time zones, and that the upset occurred about 0214 Taiwan local time, or about four to five hours after the captain had been accustomed to going to sleep. Thus, his ability to obtain, assimilate, and analyze all the data presented to him could have been impaired by the effects of monotony, boredom, and fatigue. However, an ahalysis of the captain's performance does not support a conclusion that the his performance was impaired by these factors. The facts arid circumstances showed that the captain was alert to the situation as it developed. The data also showed that the captain had five hours rest during the flight, that he had slept two hours during this period, and that he had been at his duty station about 3 hours when the upset occurred. The Safety Board concluded that the preponderance of the evidence showed that the deviations and omissions from prescribed airplane procedures noted in the captain's performance resulted from the causal factors cited earlier, i.e., distraction and over-reliance on the autopilot.
In conclusion, the Safety Board believes that the loss of thrust on the No. 4 engine was the precipitating factor in the accident; however, we do not believe that it should be considered a contributory factor. Except on takeoff, at, or shortly after critical engine failure speed, an engine loss does not require an emergency procedure wherein -immediate and memory actions are required of the flightcrew. An engine loss at cruise altitude and at cruise speeds does not place the airplane in im mediate jeopardy nor, for the most part, are any immediate responses required of the flightcrew to retrieve the airplane from jeopardy. The facts of this accident confirm this evaluation since the loss of control did not occur until more than 3 minutes after the No. 4 engine had lost thrust. More than enough time was available to the flightcrew to react properly and prevent the upset. This fact was amply demonstrated on two previous flights for this airplane in which similar situations occurred; the malfunctions were corrected, and the airplane proceeded to scheduled destinations without further incident.
The Safety Board is aware of present and proposed National Aeronautics and Space Administration (NASA) studies on the effects of circadian desynchronosis on flightcrew performance and efficiency. NASA has recently concluded a study of the effect of circadian desynchronosis on the performance of flightcrews engaged in shorthaul flights, but has not, to date, released its findings. A similar study on the effects circadian desynchronosis may have on the performance of flightcrews engaged in longhaul transmeridional flights was begun recently. Until the results of either or both of these NASA studies are released, the Safety Board believes that it would be premature to
formulate any recoin mendations which address either the effects of circadian desynchronosis on flightcrew performance or which contain actions designed to counteract these effects based solely on the results of this investigation.
Although the Safety Board was unable to identify any problems associated with the lack of crew coordination during its analysis of the accident, it also believes the facts and circumstances surrounding the upset illustrate the many factors which can complicate the problems of a multiengine airplane's flightcrew during an inflight abnormality or emergency. The Safety Board believes that the ability of a flightcrew to identify correctly the nature of an emergency or abnormality and then to cope successfully with the identified mishap can be improved and facilitated by proper crew coordination. We also believe that the full benefits of proper crew coordination can only be achieved when the captain recognizes and makes full use of the resources available to him in his cockpit; i.e. the knowledge and training of his crew members. In order to train captains and crew members to recognize these resources and to utilize them to the fullest extent possible, the Safety Board has recoin mended that the FAA develop and implement a training
program to accomplish this goal 21/. The Safety Board urges the FAA to complete the development of this program and to disseminate it to the industry.
3.1 Findings
2. The changing airspeeds encountered by Flight 006 and the resultant compensating throttle adjustments were caused by wind speed variations.
3. The No. 4 engine did not flame out, but "hung" at about 1.0 EPR.
4. During his attempt to recover the No. 4 engine, the flight engineer did not close the bleed air valve switch before advancing the No. 4 throttle.
5. The other three engines did not lose thrust nor did they flame out.
6. The captain did not disengage the autopilot in a timely manner after thrust was lost on the No. 4 engine. The autopilot effectively masked the approaching onset of the loss of control of the airplane.
7. The captain was distracted from his flight monitoring duties by his participation with the flight engineer in the evaluation of the No. 4 engine's malfunction.
8. With the exception of the loss of thrust on the No. 4 engine, no other airplane malfunction affected the performance of the airplane; the loss of thrust on the No. 4 engine did not contribute to the accident.
9. The captain was also distracted by his attempts to arrest the airplane's decreasing airspeed, and this also contributed to his failure to detect the airplane's increasing bank angle.
11. The damage to the airplane was a result of the acceleration forces and high airspeeds that occurred during the upset and recovery maneuvers.
3.2 Probable Cause
The National Transportation Safety Board determines that the probable cause of this accident was the captain's preoccupation with an inflight malfunction and his failure to monitor properly the airplane's flight instruments which resulted in his losing control of the airplane.
Contributing to the accident was the captain's over-reliance on the autopilot after the loss of thrust on the No. 4 engine.
Parties to the investigation were the Federal Aviation Administration, the Boeing Commercial Airplane Company, and the Pratt and Whitney Division of the United Technologies Corporation. The Chinese Civil Aeronautics Administration appointed an accredited representative to assist the Safety Board during the investigation. The accredited representative was assisted by advisors from China Airlines.
2. Public Hearing
There was no public hearing nor deposition proceeding.
Since N4522V was a United States (U.S.) registered airplane leased by China Airlines, the flightcrew members were required to have and did have special purpose U.S. pilot and flight engineer certificates issued under the authority of 14 CFR 61.77. These certificates authorized the pilot and flight engineer to perform flight duties "on a civil airplane of U.S. registry, leased to a person not a citizen of the United States, carrying persons or property for compensation or hire." The regulation states, in part, that these special certificates will be terminated when:
The flightcrew members on Flight 006 all possessed valid special purpose U.S. flight certificates.
The primary flightcrew consisted of Captain Mm-Yuan Ho, First Officer Ju Yu Chang, and Flight Engineer Kuo-Pin Wei; the augmentees were Captain Chien-Yuan Liao and Flight Engineer Shih Lung Su. At the time of the in-flight upset, the primary flightcrew was on duty.
Captain Min-Yuan Ho, 55, qualified as captain on Boeing 747 aircraft on May 7, 1980. He held Airline Transport Certificate No. 2319601 with an airplane multiengine land rating and a Boeing 747 type rating. His first class medical certificate was issued January 4, 1985, and he was required to "wear correcting glasses while executing the privileges of his airman certificate."
Captain Ho had passed his last two simulator proficiency checks on February 2 and November 5, 1984, and he passed his last route check on April 14, 1984. The captain had flown 15,494 hours, 3748 of which were in Boeing 747 airplanes. During the last 90 days, 30 days, and 24 hours before the accident he had flown 254 hours, 82 hours, and zero hours, respectively. At the time of the accident, the captain had been on duty about 11 hours, and 9 hours 48 minutes of this were flight time. During the flight, the captain had been relieved by the augmentee captain and had been off-duty for about 5 hours. He had resumed his captain's duties about 2 hours before the accident. In addition, the captain had been off duty 15 hours 20 minutes before reporting for duty on the accident flight.
First Officer Ju-Yu Chang, 53, qualified as first officer on Boeing 747 aircraft on August 31, 1981. The first officer held Airline Transport Pilot Certificate No. 2323152 with airplane multiengine land and Boeing 747 type ratings. His first class medical certificate was issued November 15, 1984, with no limitations.
The first officer had passed his last two simulator proficiency checks on April 23, 1984 and November 23, 1984, and his last route check on June 7, 1984. The first officer had flown 7,734 hours, 4,553 of which were in Boeing 747 airplanes. During the last 90 days, 30 days, and 24 hours before the accident, he had flown 251 hours, 67 hours, and zero hours, respectively. At the time of the accident the first officer had been on duty about 11 hours, of which 9 hours and 48 minutes were flight time. During the flight, the first officer had been off duty about 3 hours and had resumed his first officer's duties about 3 hours before the accident. In addition, the first officer had been off duty about 26 hours before reporting for the accident flight.
Flight Engineer Kuo-Pin Wei, 55, qualified as a Boeing 747 flight engineer on August 13, 1979. He held Flight Engineer Certificate No. 2319358 with turbojet powered and Boeing 747 type ratings. The flight engineer's first class medical certificate was issued December 17, 1984, and he was required to "wear correcting glasses while exercising the privileges of his airman's certificate."
The flight engineer had passed his last two simulator proficiency checks on October 26, 1983 and May 21, 1984, and his last two route checks on August 9, 1984 and December 18, 1984. The flight engineer had flown 15,510 hours, 4,363 of which were in Boeing 747 airplanes. During the last 90 days, 30 days, and 24 hours before the accident, he had flown 235 hours, 96 hours, and zero hours. At the time of the accident he had been on duty about 11 hours, and 9 hours 48 minutes of this were flight time. During the flight, the flight engineer was off about 5 hours and had resumed his flight engineer's duties about 2 hours before the accident. In addition, the flight engineer had been off duty about 93 hours before reporting for the accident flight.
The two augmentee flightcrew members, Captain Chien-Yuan Liao, 53, and Flight Engineer Po-Chae Su Shih Lung, 41, were certificated properly, held valid medical certificates, and had received and passed all required flight and simulator checks.
Boeing 747 SP-09, N4722V
The airplane, manufacturer's serial No. 22805, was delivered to China Airlines June 29, 1982, and has been operated continuously by China Airlines since that date. At the time of the accident, the total airframe time was 10,192 hours 51 minutes. Except for the writeups relating to the No. 2 engine, an examination of the airplane logbook for the last 30 days disclosed no data which could be characterized as other than routine.
The airplane was powered by four Pratt & Whitney JT9D-7A engines rated at 46,150 pounds of thrust for takeoff. The following statistical data were compiled:
Powerplants
| Engine | No. 1 | No. 2 | No. 3 | No. 4 | |
| Serial No. | 695816 | 695737 | 695725 | 695796 | |
| Date of Installation | 12-13-84 | 10-26-84 | 10-22-84 | 11-03-84 | |
| Total Time | 10,518:02 | 21,759:10 | 20,931:09 | 12,742:53 | |
| Total Cycles | 1,954 | 4,385 | 4,358 | 3,097 |